

Effects of Bisphenol A on Incidence and Severity of Cardiac Lesions in the NCTR-Sprague-Dawley rat: A CLARITY-BPA Study
Robin Gear, Jessica A. Kendziorski, and Scott M. Belcher.
Toxicology Letters (2017)
DOI: https://doi.org/10.1016/j.toxlet.2017.05.011
PMID: 28499613
Publication
Abstract
The goal of this study was to determine whether bisphenol A (BPA) had adverse effects indicative of cardiac toxicity. As part of the "Consortium Linking Academic and Regulatory Insights on BPA Toxicity" (CLARITY-BPA), study dams and offspring were exposed by daily gavage to five doses of BPA ranging from 2.5 to 25000μg/kg/day, 0.05 or 0.5μg/kg/day 17α-ethinyl-estradiol (EE) or 0.3% carboxymethylcellulose vehicle. Exposure-related effects were analyzed in isolated hearts by quantitative morphometry and histopathology. No dose-related changes in body weight were detected. Across all exposure groups including vehicle controls, body weight of continuously dosed males was reduced compared to males dosed only until PND21. Heart weight was increased only in females exposed to EE, and consistent alterations in LV wall thickness were not observed. Exposure-related changes in collagen accumulation were minor and limited to highest EE exposure groups with increased collagen accumulation in PND21 males. Decreased collagen was observed in hearts of BPA or EE exposed females at PND90 and PND180. In BPA or EE treated females cardiomyopathy incidence and severity was significantly increased compared to control females at PND21 with myocardial degeneration observed in both males and females at PND21 and PND90.
Figures
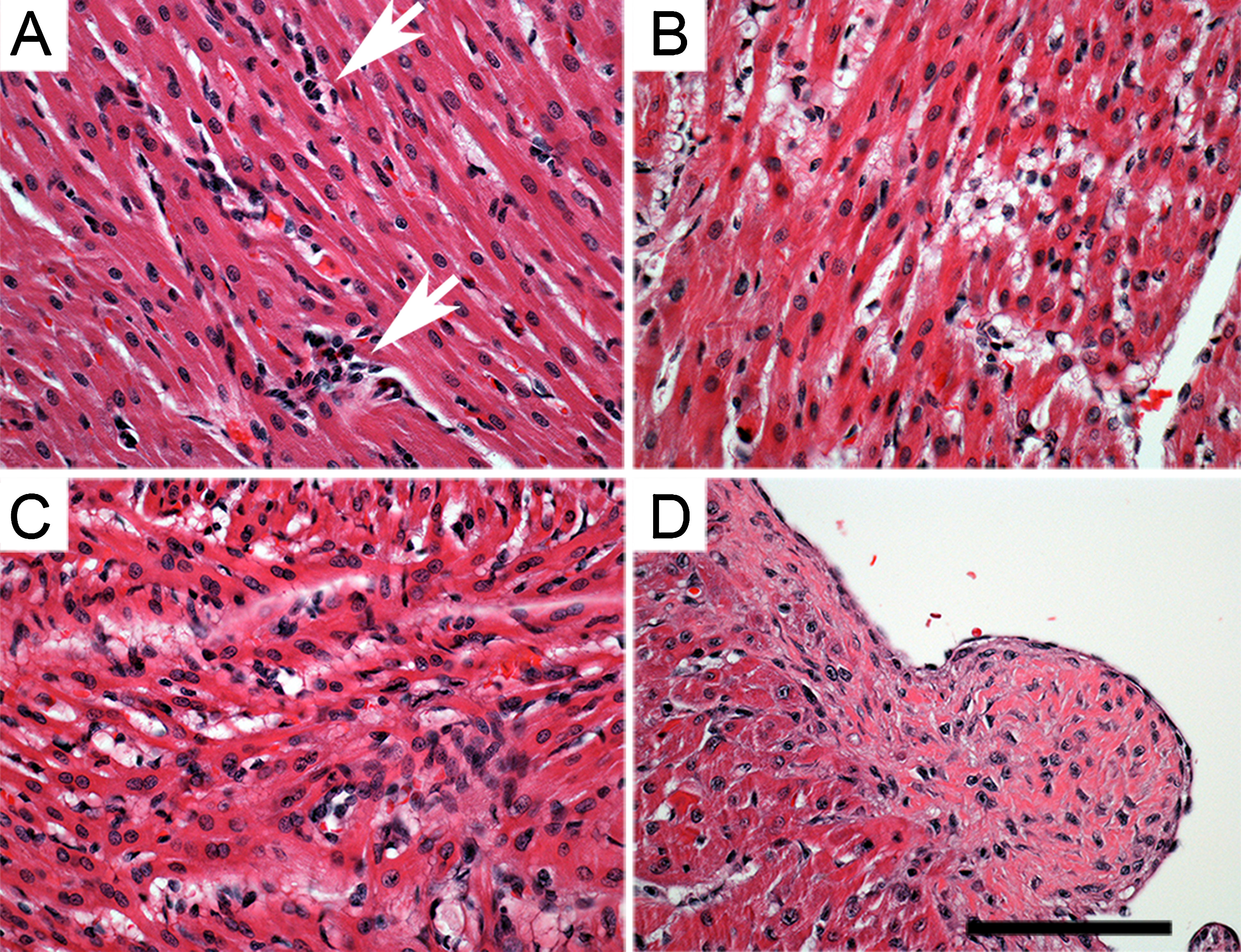
Figure 1. Cardiomyopathy at PND21.
Small regions of inflammatory cell infiltrates (white arrows) indicative of the earliest stages of cardiomyopathy (A).
Areas of myocyte degeneration with extensive vacuolation of myocytes and lacking evident fibrosis (B).
Small regions of mid-stage PCM with highly disorganized myocyte morphology, evident myocyte degeneration, diffuse vacuolation, increased cellularity and fibrosis (C).
Focal fibrosis indicative of late stage cardiomyopathy (D).
Bars = 100 μm.
- Figure 1 (2 MB)
{kind=link}
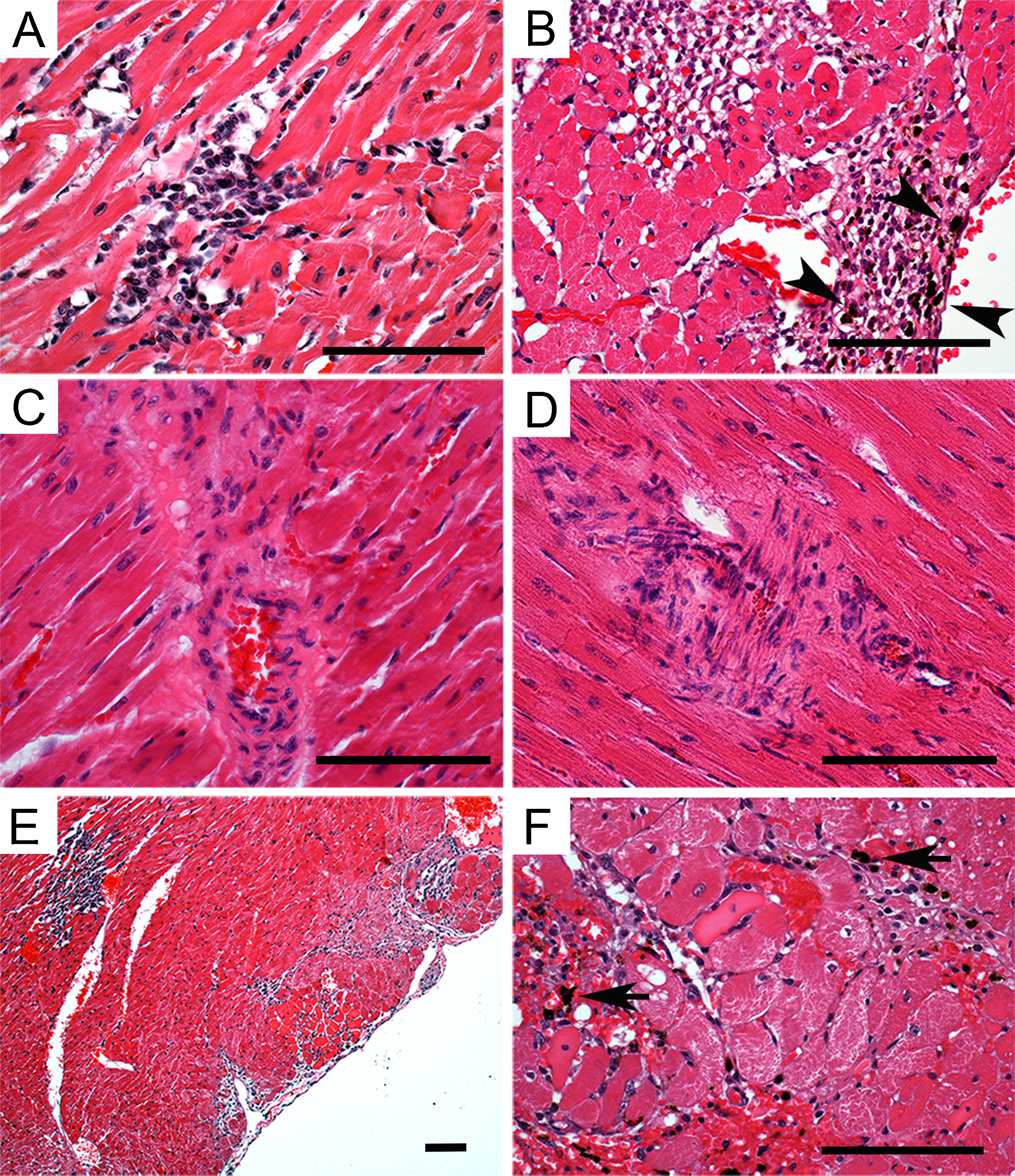
Figure 2. Cardiomyopathy at PND90 and 6 months.
Lesions at PND90 were characterized by degenerating myofibrils associated focal and multifocal inflammatory cell infiltrates (A).
Regions of extensive myocyte necrosis with inflammatory cell infiltrates and hemosiderin containing macrophages (B; arrowheads).
Focal perivascular and interstitial fibrosis indicative of late-stage cardiomyopathy in control female (C) and male (D) at PND90.
At 6 months cardiomyopathy at this age was characterized by multifocal lesions with a larger area of involvement (E).
Evident degenerating myofibrils associated focal and multifocal inflammatory cell infiltrates with hemosiderin containing macrophages (arrows) suggestive of previous vascular hemorrhage were also observed (F).
Bars = 100 μm.
- Figure 2 (4 MB)
{kind=link}
Tables
Table 1. Male and Female Body Weight (g).
- Table 1 (32 KB)
Table 2. Male and Female Heart Weight (mg).
- Table 2 (38 KB)
Table 3. Male and Female Heart Weight/Body Weight (mg/g).
- Table 3 (40 KB)
Table 4. Male and Female LV Wall thickness (mm).
- Table 4 (32 KB)
Table 5. Male and Female Fibrosis (percentage of LV Area).
- Table 5 (32 KB)
Table 6. Incidence of Cardiac Lesions at PND 21.
- Table 6 (47 KB)
Table 7. Incidence of Cardiac Lesions at PND90.
- Table 7 (38 KB)
Table 8. Incidence of Cardiac Lesions at 6 Months.
- Table 8 (42 KB)